Y-Chromosome Microdeletion Testing
Y-Chromosome Microdeletion Testing in Male Infertility: Why a Very Low Sperm Count Needs Deeper Evaluation
A semen analysis is often the first test performed when a couple is finding it difficult to conceive. When the report shows an extremely low sperm concentration – or no sperm at all – it can be distressing.
However, this result is not a judgment about masculinity, and it does not automatically mean that biological parenthood is impossible. It is a clinical clue that deserves a careful search for the underlying cause.
One important cause is a Y-chromosome microdeletion: a very small missing segment of genetic material from the Y chromosome. These deletions can remove genes required for sperm production.
Identifying a microdeletion can:
- • Explain why sperm production is severely reduced
- • Help estimate whether sperm might be found in the testes
- • Guide decisions about surgical sperm retrieval
- • Support planning for IVF with intracytoplasmic sperm injection—ICSI
- • Provide important information for genetic counselling
What is a Y-chromosome microdeletion?
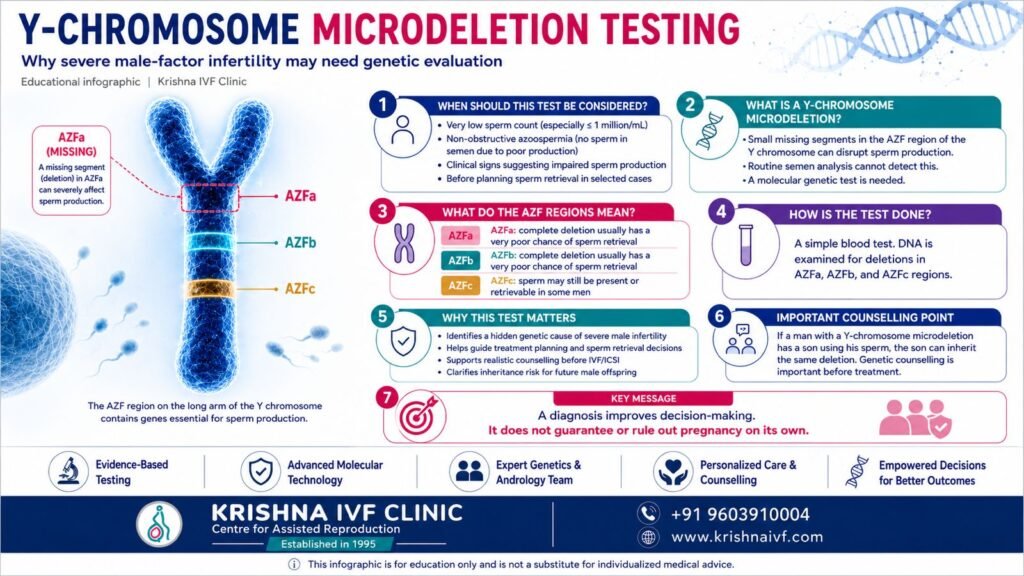
Most men have one X chromosome and one Y chromosome. On the long arm of the Y chromosome, called Yq, lies an area known as the azoospermia factor—or AZF—region.
The AZF region is divided clinically into three principal areas:
- • AZFa
- • AZFb
- • AZFc
These regions contain genes that are important for the formation and maturation of sperm.
A microdeletion means that a small segment of DNA within one or more of these regions is absent. It is usually too small to be detected by a routine chromosome test called a karyotype. A dedicated molecular genetic test is therefore required.
The European Academy of Andrology and EMQN recommend a validated multiplex polymerase chain reaction—PCR—method, followed when necessary by more detailed deletion-extension analysis, to detect and correctly define clinically important AZF deletions.
Y-chromosome microdeletions are most often identified in men with non-obstructive azoospermia or severe oligozoospermia. They are uncommon when the sperm concentration is above 5 million/mL. The deletion is usually present from conception. It is not caused by stress, sexual activity, diet or anything that the patient or partner has done.
Who should consider this test?
Current guidelines consider both sperm concentration and evidence of impaired sperm production when deciding who should be tested.
The European Association of Urology recommends Y-chromosome microdeletion testing in men with a sperm concentration of 1 million/mL or less. Testing may also be considered when the sperm concentration is below 5 million/mL, depending on the clinical findings.
The 2024 AUA/ASRM guideline recommends testing men with primary infertility who have:
- • Azoospermia, or
- • A sperm concentration of 1 million/mL or less
This recommendation particularly applies when there is elevated follicle-stimulating hormone—FSH—small testes or another diagnosis suggesting impaired sperm production.
Testing is therefore particularly relevant in men with:
- • Non-obstructive azoospermia
- • Severe oligozoospermia, especially at or below 1 million sperm/mL
- • Very low sperm counts accompanied by elevated FSH
- • Reduced testicular volume
- • Suspected testicular sperm-production failure
- • Planned surgical sperm retrieval
- • A clinical situation in which a genetic diagnosis would change treatment or counselling
A failed IVF or ICSI cycle alone is not an automatic indication for Y-microdeletion testing. A failed treatment cycle should prompt a structured review of both partners, but this genetic test is selected mainly according to semen findings, examination, hormone levels and the suspected cause of male infertility.
How is the test performed?
Y-chromosome microdeletion analysis usually requires a small blood sample.
DNA is extracted from the sample and examined for specific genetic markers within the AZFa, AZFb and AZFc regions. A clinically useful report should clearly state:
• Which AZF region is affected
• Whether the deletion is complete or partial
• Whether more detailed characterisation is required
• What the result may mean for sperm production and retrieval
Testing should be undertaken in a molecular genetics laboratory using validated methods, appropriate positive and negative controls and recognised quality-assurance procedures. Standardisation is important because incorrect or incomplete interpretation can lead to inappropriate counselling or unnecessary surgery.
Y-microdeletion analysis is not the same as:
- • Semen analysis, which evaluates sperm concentration, movement and morphology
- • Karyotyping, which detects larger chromosome abnormalities
- • Sperm DNA-fragmentation testing, which evaluates DNA damage within sperm
- • General carrier screening, which looks for selected inherited disorders
In severe oligozoospermia or azoospermia, more than one genetic investigation may be appropriate. Karyotyping may be advised alongside Y-chromosome testing. Hormonal evaluation, clinical examination, repeat semen analysis and imaging when indicated also remain important.
The World Health Organization emphasises standardised semen examination, while the EAU recommends at least two consecutive semen analyses when the first test is abnormal.
Why does the exact AZF region matter?
A Y-chromosome microdeletion result should not be interpreted simply as “positive” or “negative.” The exact region involved strongly influences the prognosis.
Complete AZFa deletion
A complete AZFa deletion is usually associated with severe failure of sperm-cell development. Testicular tissue commonly shows a Sertoli-cell-only pattern, in which the supporting cells are present but sperm-forming germ cells are absent.
The probability of finding sperm through testicular surgery is close to zero. Current European guidance recommends against testicular sperm extraction when there is a complete AZFa deletion.
Complete AZFb deletion
A complete AZFb deletion is generally associated with maturation arrest. Early germ cells may be present, but they do not progress into mature sperm.
As with complete AZFa deletion, the likelihood of successful sperm retrieval is extremely poor. Identifying this deletion before surgery can help a patient avoid an invasive procedure that has almost no realistic chance of success.
AZFc deletion
AZFc is the most frequently identified classical AZF deletion.
Its clinical expression is variable. Some men have a very low sperm count, while others have azoospermia. Unlike complete AZFa or AZFb deletions, sperm may still be found in the ejaculate or retrieved from testicular tissue.
The EAU guideline reports that testicular sperm may be found in approximately 50%- 75% of men with AZFc microdeletions. This range describes groups of patients and should not be interpreted as a guaranteed result for an individual man.
When sperm are present in the ejaculate, sperm freezing may be discussed. In men with non-obstructive azoospermia, microdissection testicular sperm extraction—micro-TESE—may be considered after detailed evaluation and counselling.
When only very small numbers of sperm are available, the retrieved sperm would usually need to be used with ICSI.
Combined and partial deletions
Combined deletions, such as AZFbc or deletions extending across multiple AZF regions, generally have a poorer prognosis.
Partial deletions require especially careful interpretation. Their clinical significance may vary according to the exact genetic change, the affected genes and the person’s Ychromosome population background. A “partial deletion” should therefore not automatically be treated as equivalent to a complete classical AZF deletion.
Can a man with an AZF deletion have a biological child?
Sometimes, yes. The possibility depends mainly on the deletion type and whether usable sperm are present or can be retrieved.
Men with complete AZFa or complete AZFb deletions are very unlikely to have retrievable sperm. Alternative family-building pathways may therefore need to be discussed sensitively.
Men with AZFc deletions have a more favourable possibility of finding sperm. However, the eventual chance of pregnancy is also influenced by:
- • The female partner’s age
- • Ovarian reserve
- • Oocyte number and quality
- • Embryo development
- • Uterine and endometrial factors
- • The health and reproductive history of both partners
ICSI can permit fertilisation using a single viable sperm, but it does not repair the genetic deletion. It also cannot guarantee fertilisation, blastocyst development, pregnancy or live birth.
Evidence regarding assisted-reproduction outcomes in men with AZFc deletions remains mixed. Some studies report reduced fertilisation rates, while the effect on live birth is less certain. Results should therefore be discussed in a balanced and individualised manner rather than presented as one universal percentage.
Will the deletion be passed to the child?
The Y chromosome passes from father to son. Therefore, when a male child is conceived using sperm from a man with a Y-chromosome microdeletion, the son will inherit the deletion.
A daughter does not inherit her father’s Y chromosome.
The principal expected implication for a son is a future risk of impaired sperm production. However, the severity may not be identical to that of the father. The son could develop a very low sperm count or azoospermia when he reaches reproductive age.
This is why pre-treatment genetic counselling is essential.
Counselling should explain:
- • How the deletion is inherited
- • What is known and uncertain about future male offspring
- • The chance of retrieving sperm
- • The role and limitations of ICSI
- • The available reproductive alternatives
- • The ethical and legal framework applicable in India
The purpose of counselling is not to create fear. It is to help the couple make a well informed decision that reflects their medical situation, values and preferences.
What the result cannot tell us
Y-chromosome microdeletion testing can identify a cause and improve treatment planning, but it cannot:
- • Guarantee that sperm will or will not be retrieved in every man
- • Predict embryo quality in a particular IVF cycle
- • Measure sperm DNA fragmentation
- • Explain every case of severe oligozoospermia or azoospermia
- • Guarantee pregnancy after IVF or ICSI
- • Replace evaluation of the female partner
Male and female fertility should be assessed in parallel. This is particularly important when the female partner is older or has reduced ovarian reserve, because the available reproductive time may influence whether clinicians recommend further investigations, sperm retrieval, sperm preservation or assisted reproduction.
A more precise path forward
A very low sperm count should not lead immediately to treatment without an appropriate diagnosis.
A structured male-fertility assessment can:
- • Distinguish obstruction from impaired sperm production
- • Identify hormonal or genetic causes
- • Avoid procedures that are unlikely to help
- • Clarify whether sperm retrieval should be attempted
- • Support realistic reproductive planning
At Krishna IVF, Y-chromosome microdeletion analysis is considered as one component of a broader male-infertility evaluation rather than as an isolated test.
Semen findings, medical and reproductive history, examination, hormone levels, imaging when appropriate, karyotype results and the couple’s complete reproductive situation should be reviewed together. When a deletion is identified, its meaning should be explained in clear language, including its implications for sperm retrieval, ICSI, inheritance and alternative reproductive pathways.
The central message is one of precision, not pessimism.
A genetic diagnosis may not change the underlying biological condition, but it can prevent unnecessary interventions, guide responsible use of reproductive technology and help couples make informed and ethically sound decisions.
Medical disclaimer : This article is intended for general education and information. It does not provide an individual diagnosis or treatment recommendation. Genetic testing and fertility-treatment decisions require personalised consultation with a qualified fertility specialist, andrologist or reproductive genetic counsellor.
References
- European Association of Urology. EAU Guidelines on Sexual and Reproductive Health: Male Infertility. EAU Guidelines Office; 2026.
- American Urological Association; American Society for Reproductive Medicine. Diagnosis and Treatment of Infertility in Men: AUA/ASRM Guideline. Published 2020; amended 2024.
- World Health Organization. WHO Laboratory Manual for the Examination and Processing of Human Semen. 6th ed. World Health Organization; 2021.
- Krausz C, Navarro-Costa P, Wilke M, Tiittelmann F. EAA/EMQN best practice guidelines for molecular diagnosis of Y-chromosomal microdeletions: state of the art 2023. Andrology. 2023. doi:10.1111/andr.13514.
- Golin AP, Yuen W, Flannigan R. The effects of Y chromosome microdeletions on in vitro fertilization outcomes, health abnormalities in offspring and recurrent pregnancy loss. Transl Androl Urol. 2021;10(3):1457-1466. doi:10.21037/tau-19-672.