Sperm Freezing
Sperm freezing, also referred to as sperm cryopreservation, is a laboratory-based reproductive preservation procedure utilized in selected fertility evaluation and assisted reproductive treatment workflows.
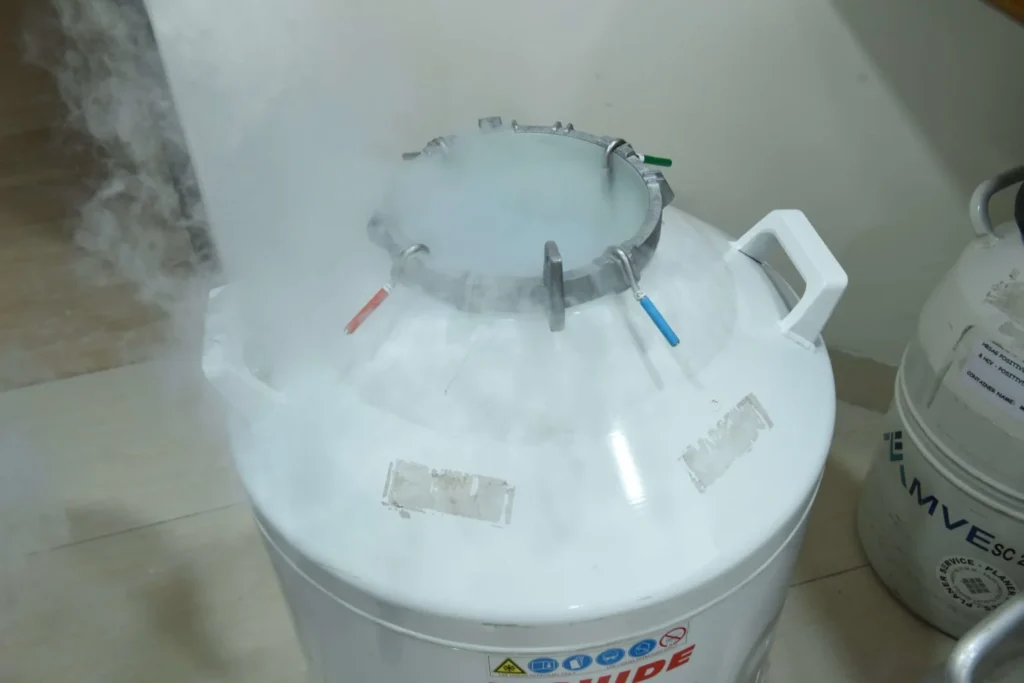
Cryopreservation involves storage of sperm samples at very low temperatures using controlled laboratory protocols and cryoprotective media designed to support preservation of sperm viability during freezing and thawing procedures.
Sperm cryopreservation may be considered in selected clinical situations including fertility preservation before medical or surgical treatments, assisted reproductive treatment planning, selected male infertility conditions, difficulty in sperm collection on the day of treatment, or other reproductive indications where clinically appropriate.

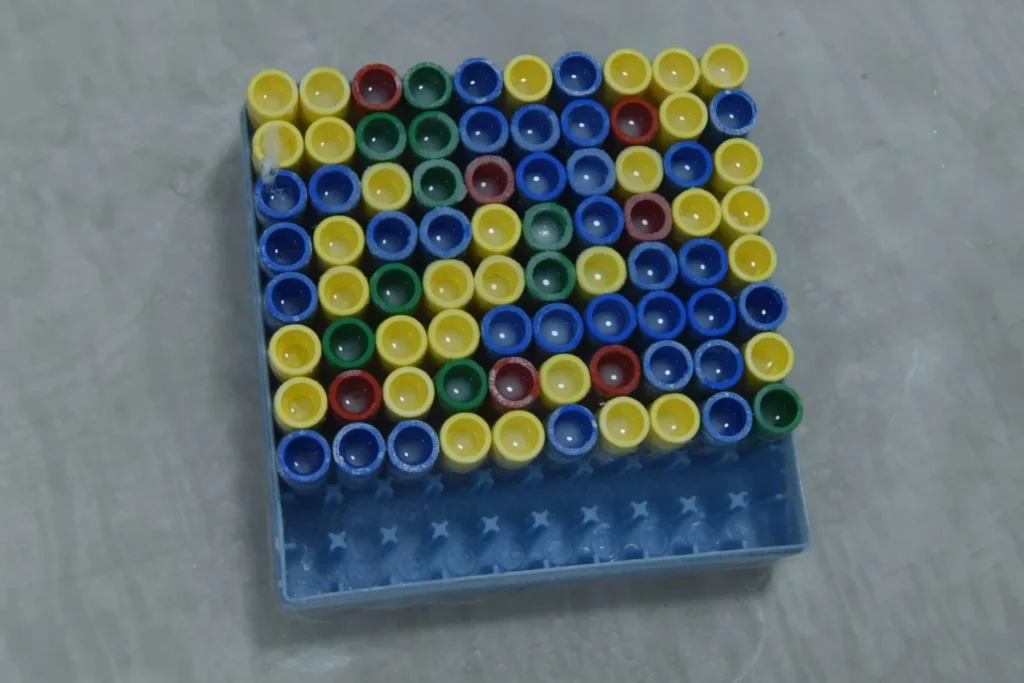
Laboratory cryopreservation workflows may include semen analysis, sperm preparation, sample identification, documentation, controlled freezing procedures, cryostorage protocols, and thawing procedures depending on clinical and laboratory requirements.
Cryopreservation techniques and laboratory protocols are designed to reduce cellular damage associated with freezing and thawing processes. Post-thaw sperm quality may vary depending on the initial semen parameters, laboratory methods, and individual biological factors.
Fertility preservation counseling and cryopreservation planning may form part of reproductive treatment workflows in selected patients undergoing medical treatments that could affect future fertility potential.
Sperm freezing at Krishna IVF forms part of broader clinical embryology, reproductive laboratory, and fertility preservation workflows within individualized reproductive medicine protocols.
Research activities related to cryopreservation and embryology workflows from Krishna IVF have contributed to published scientific literature in reproductive medicine.